Welcome to Calvary Robotics
A global leader in crafting tailor-made turnkey automation solutions, robotics platforms, and material handling systems. Boasting over 30 years of expertise and a team of 280+ professionals across four specialized business units, we’re unmatched in the field. Our strength lies in our extensive experience and seamless unit synergy. Calvary offerings encompass system design, manufacturing, tooling, and commercialization, backed by a sophisticated project management system that ensures clear communication and procedural precision. Prioritizing customer satisfaction, we emphasize security and confidentiality through rigorous practices. Our reputation stands as a testament to the enduring partnerships we build. Welcome to a realm of quality, performance, and service – welcome to Calvary Robotics.



.jpg?width=300&name=Homepage%20Image%20-%20(Energy).jpg)
Green Tech
Optimize your energy operations with our industrial automation systems, minimizing downtime and maximizing output.
Read MoreGreen Tech
Optimize your energy operations with our industrial automation systems, minimizing downtime and maximizing output.
Read More.jpg?width=300&name=Homepage%20Image%20-%20(Consumer%20Products).jpg)
Consumer Products
Accelerate your manufacturing process, reduce costs, and bring products to market faster with our state-of-the-art automation and robotics technology.
Read MoreConsumer Products
Accelerate your manufacturing process, reduce costs, and bring products to market faster with our state-of-the-art automation and robotics technology.
Read More
Industrial
Optimize your production efficiency, reduce operational costs, and stay ahead in the competitive market by adopting sustainable, technologically advanced manufacturing practices.
Read MoreIndustrial
Optimize your production efficiency, reduce operational costs, and stay ahead in the competitive market by adopting sustainable, technologically advanced manufacturing practices.
Read More.jpg?width=300&name=Homepage%20Image%20-%20(Healthcare%20&%20Medical).jpg)
Life Sciences
Improve patient care, enhance medical research, and increase efficiency in life sciences settings with our cutting-edge robotics and automation solutions.
Read MoreLife Sciences
Improve patient care, enhance medical research, and increase efficiency in life sciences settings with our cutting-edge robotics and automation solutions.
Read More
Transportation
Streamline your production line, enhance quality control, and boost productivity with our innovative robotic automation solutions.
Read MoreTransportation
Streamline your production line, enhance quality control, and boost productivity with our innovative robotic automation solutions.
Read MoreCalvary Robotic Platforms
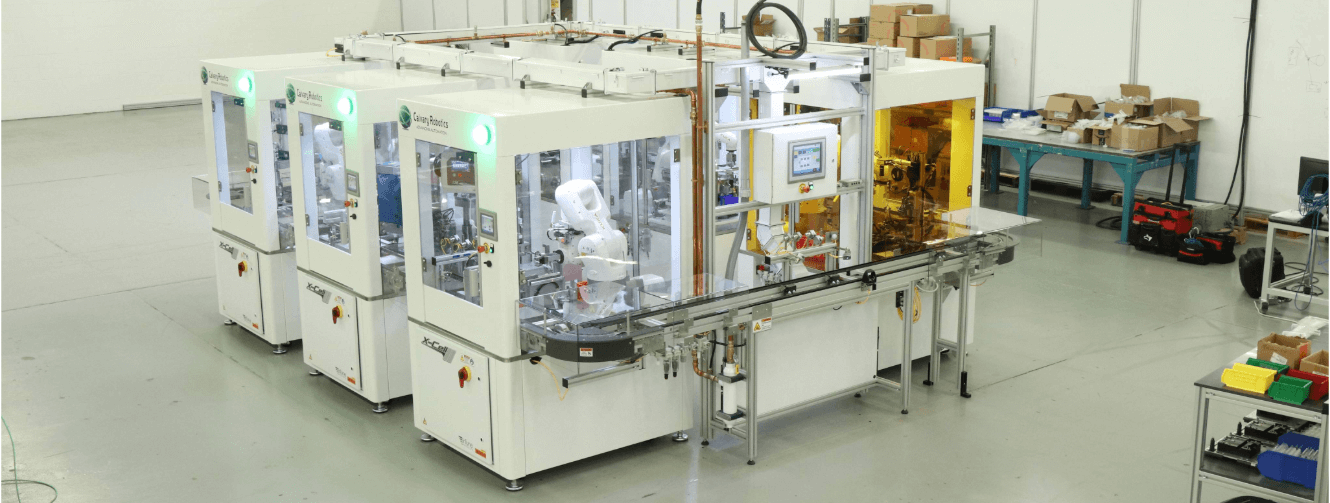
- X-Cell Series
- Flexible Manufacturing Systems
- Flexible Feeding & Sorting
- Machine Tending
- Robotic Software Platforms

.jpg?width=300&name=Homepage%20Image%20-%20(Calvary%20Robotics%20Platforms%20-%20Flexible%20Manufacturing%20Systems).jpg)
.webp?width=300&name=Homepage%20Image%20-%20(Calvary%20Robotics%20Platforms%20-%20Flexible%20Feeding%20&%20Sorting).webp)
.jpg?width=300&name=Homepage%20Image%20-%20(Calvary%20Robotics%20Platforms%20-%20Machine%20Tending).jpg)
.jpg?width=300&name=Homepage%20Image%20-%20(Calvary%20Robotics%20Platforms%20-%20Robotic%20Software%20Platforms).jpg)
- Automotive & Transportation
- Consumer Products
- Electronics
- Energy
- Food & Beverage
- Healthcare & Medical
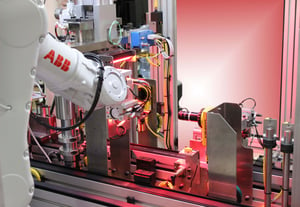
Automotive & Transportation Automation: Streamline your production line, enhance quality control, and boost productivity with our innovative robotic automation solutions.
At Calvary, we have a rich history of serving the automotive industry, making us one of the leading automation and robotics companies in the market. Our expertise spans a diverse range of technology applications, including semi-automated lean cells, robotic work cells, asynchronous and synchronous assembly systems, flexible platform technology, web handling, functional test, and inspection systems.
Our team is well-versed in various control systems and data analysis software platforms, enabling us to deliver efficient and precise solutions for your automation needs. Additionally, Calvary excels in integrating third-party equipment and systems seamlessly into our final solutions, ensuring a comprehensive and unified approach to your automation projects.
We understand the importance of handling cost and delivery constraints effectively. Through innovative solutions and close collaboration with our customers, we have successfully tackled complex challenges while delivering projects on time and within budget. Our team is fully acquainted with customer expectations, including statistical quality metrics (Cpk, gauge R&R, capability studies), robust tooling design, poka-yoke verification methods, lean manufacturing practices, and just-in-time production.
At Calvary, we are your one-stop shop for all core technologies, offering expertise in robotics, feeding, part placement, assembly methodologies, joining technologies, dispensing, inspection, testing, material handling, and packaging solutions. Whatever your automotive automation requirements, we have the solution.
Specialized Applications:
- Emission Control Products
- Sensors and Actuators
- Electronics and Associated Assemblies
- Safety Products
- Control Modules
- Engine Management Components
- Fuel Delivery Systems
- Braking Systems
- Steering Systems
- Thermal Management Products
When it comes to industrial robotic system integration for the automotive industry, Calvary stands out as a trusted partner that delivers innovation, efficiency, and reliability. Partner with us today to take your automotive manufacturing processes to the next level!
Consumer Products Automation: Accelerate your manufacturing process, reduce costs, and bring products to market faster with our state-of-the-art automation and robotics technology.

With extensive experience spanning a wide range of products, Calvary Robotics has established itself as a leading automation and robotics company in the Consumer Products industry. Our expertise includes the utilization of multiple technologies to optimize processes for both high-volume and high-mix production scenarios. Furthermore, we take pride in offering solutions that accommodate flexible volumes through the design of modular and scalable systems.
We understand the significance of ongoing product development and design iterations in the consumer products sector. Our solutions are carefully tailored to handle delicate product handling, ensuring that cosmetic damage is avoided for products that will be exposed to end users.
At Calvary Robotics, we have successfully worked with various controls platforms and have seamless integration experience with ERP and MES systems, as well as plant floor supervisory networks. Our robust controls capabilities facilitate batch and part-level data collection, enabling efficient tracking, analysis, and record-keeping processes.
We excel at integrating a wide array of technologies commonly used in consumer products manufacturing. From feeding and filling to coating, dispensing, screw driving, welding technologies, electronic, leak, and functional testing, vision inspection, marking processes, and primary and secondary packaging operations – we’ve got you covered.
Specialized Applications:
- Consumer Electronics
- Optical and Electronic Connectors
- Household Goods
- Small and Large Appliances
- Lawn and Garden
- Office Products
- Toiletries
Calvary Robotics has consistently provided innovative solutions for various consumer product applications. As a reliable partner, we are dedicated to delivering automation and robotic integration solutions that drive efficiency, quality, and productivity for your consumer products manufacturing processes.
Electronics Automation: Stay ahead in the rapidly evolving electronics industry by leveraging our expertise in robotic integration for increased precision and efficiency.

As a leading automation and robotics company, Calvary has a remarkable track record of delivering world-class Electronics Assembly systems to some of the foremost manufacturing companies in the industry. Our extensive experience covers the seamless integration of various technologies and applications used globally today, making us a preferred choice for electronics manufacturing.
Our expertise extends to the integration of PCB manufacturing equipment, soldering/welding, functional testing, part marking, traceability, calibration, coating and sealing systems, and component assembly, among other cutting-edge technologies. At Calvary, we ensure that your electronics assembly process is optimized for efficiency, precision, and quality.
We pride ourselves on being well-versed with the requirements, environment control, ESD practices, and SMEMA interfacing, ensuring that your electronics assembly operations adhere to the highest industry standards.
Specialized Applications:
- Electronic Actuators
- Sensors and Actuators
- Connectors
- Control Modules
- Meters and Displays
- Computer Peripherals
- PDA and Smartphone Components
- Energy Storage Devices/Batteries
- Integration of Standard Electronic Assembly and Test Equipment
Calvary Robotics has successfully provided innovative solutions for a diverse range of specialized applications in the electronics industry. Our expertise in electronics assembly and integration ensures that your manufacturing processes are equipped to meet the demands of today’s dynamic market.
Partner with Calvary today to elevate your electronics assembly capabilities and achieve unparalleled precision and efficiency. Let our skilled team of engineers and technicians bring cutting-edge automation and robotics solutions to your electronics manufacturing operations!
Energy Automation: Optimize your energy operations with our industrial automation systems, minimizing downtime and maximizing output.

With an impressive track record spanning many years, Calvary has been a leading provider of systems for the Energy and Storage Industry. Our expertise extends to designing and delivering state-of-the-art systems for the PV Industry, catering to both traditional polycrystalline products and thin film-based solar products. These systems are built around various material handling methodologies, including web, asynchronous conveyors, synchronous transfer dials, and chassis, as well as robotic modules, ensuring optimal efficiency and productivity.
Our team of experts is highly experienced in all aspects of solar cell and module production and handling, guaranteeing that our solutions meet the industry’s highest standards. Additionally, Calvary has successfully developed systems for battery assembly, fuel cell technology, and hybrid electric vehicle componentry, showcasing our versatility in the Energy and Storage sector.
Specialized Applications:
- Fuel Cell Manufacturing and Test
- Solar Panel Assembly and Test
- Wafer, Web, and Glass Handling
- Energy Storage
- Batteries
- Energy Transmission
- Nuclear
- Hybrid Electric Vehicles Components
At Calvary, we take pride in offering innovative solutions for various specialized applications within the Energy and Storage Industry. Whether you require cutting-edge fuel cell manufacturing and testing systems or state-of-the-art solar panel assembly and testing solutions, our team has the expertise and experience to deliver world-class results.
Partner with Calvary today to leverage our industry-leading knowledge in energy and storage systems, and propel your operations towards a more efficient and sustainable future. Let us be your trusted partner for all your energy and storage automation and robotics needs!
Food & Beverage Automation: Ensure food safety, hygiene, and consistency with our advanced robotic automation solutions designed specifically for the food and beverage industry.

As consumer demands evolve and labor challenges persist, Calvary Robotics continues to spearhead innovation in the Food and Beverage Industry. We understand the critical importance of meeting these challenges head-on and have developed cutting-edge solutions that address them effectively.
With a commitment to strict food safety guidelines and principles, Calvary employs cross-discipline design fundamentals to deliver sanitary and hygienic designs. Our solutions are designed to optimize food safety standards, ensuring your production processes comply with the highest industry regulations.
The results of implementing Calvary’s solutions are remarkable. Businesses experience increased throughput, generous Return on Investment (ROI), and improved product quality—all while minimizing floor space requirements. We take pride in developing efficient and space-saving systems that maximize your productivity and profitability.
Calvary’s competitive edge lies in our large-scale capacity and robust supply chain, allowing us to provide highly competitive machine lead times. Our prompt and efficient service ensures that your operations stay on schedule and meet market demands with ease.
Specialized Applications:
- Primary and Secondary Packaging
- Raw Protein Handling
- Variety Packages
- Pre-packaged Product
- High Throughput Production
- Quality Control; Machine Vision Inspection
- Flexible Handling Platforms
- End-of-line Palletizing
- Retail Dispensary Systems
- After Market Service and Support
At Calvary Robotics, we have successfully provided innovative solutions for a wide range of specialized applications within the Food and Beverage Industry. Whether you need efficient packaging, handling raw protein, ensuring quality control, or optimizing end-of-line palletizing, our expertise covers it all.
Partner with Calvary today to revolutionize your Food and Beverage production processes. Embrace automation and robotics to stay ahead in the market, and let our solutions drive your success in this dynamic industry!
Healthcare & Medical Automation: Improve patient care, enhance medical research, and increase efficiency in healthcare settings with our cutting-edge robotics and automation solutions.

As a trusted partner to a large number of global medical device, diagnostic, and pharmaceutical companies, Calvary Robotics has established itself as a frontrunner in delivering advanced systems for the Healthcare Industry.
Our expertise encompasses the design of systems for a diverse range of medical assemblies, including sharps products for infusion and extraction, tubing and valves, glass products, syringes, diagnostics, and medical electronic devices. These assembly and test systems incorporate a multitude of technologies, such as robotics, feeding, placement and assembly, joining, curing, inspection, material handling, testing, and packaging. Our automation solutions are based on various technology configurations, including lean cells, robotic platforms, asynchronous and synchronous transfer systems, and web-based and linear motor-based conveyance systems.
We understand the criticality of adhering to clean room equipment design, cGMP, IQ/OQ validation requirements, and associated documentation in the Healthcare Industry. Calvary collaborates closely with your team to define the division of scope between your operations and our solutions, ensuring compliance with regulatory requirements and your general practices. Our approach ensures a predictable and reliable solution that meets or exceeds your stringent requirements.
Specialized Applications:
- Sharps Products
- Syringes and Catheters
- Infusion Products
- Diagnostic Products
- Medical Electronic Devices
- Glass Products
- Lab Automation
- Pharmaceuticals
- Non-Woven and Film-Based Products
- Tube Sets
- Valving Components and Assemblies
- Machine Tending Applications
- Material Handling Systems
- Testing and Inspection Systems
- Primary and Secondary Packaging
Calvary Robotics has a proven track record of providing innovative solutions for various specialized applications within the Healthcare Industry. Whether it’s enhancing precision in medical device assembly or streamlining pharmaceutical packaging processes, our expertise spans the entire spectrum of Healthcare automation.
Partner with Calvary today to revolutionize your Healthcare Industry operations and embrace automation for enhanced efficiency, reliability, and compliance. Let us be your trusted automation partner, driving success and growth in this critical sector!




Contact Our Team Of Experts